







Introduction
Cell therapies for regenerative medicine (Regen Med) and immunotherapies such as Chimeric Antigen Receptor (CAR)-T and Tumor Infiltrating Lymphocytes (TIL) cell therapies are breakthroughs for cancer patients with similar promise shown in Regen Med trials. Unfortunately, response rates vary for Regen Med and immunotherapy trials. For example, clinical outcomes show 20-50% recurrence rates within one year for patients that receive CAR-T Therapy (Nat.Med, doi.org/10.1038/s41591-021-01436-0), indicating opportunities for greater clinical benefit. While autologous cell therapies are continuing, allogeneic cell therapies are increasing and require access to healthy donors starting material. The issue is that cellular starting material, whether from autologous or allogeneic sources, can vary substantially in its therapeutic potential because of the inherent functional status of the cells being harvested for therapeutic development and use.
Factors contributing to clinical outcome variability
Part of the variability in clinical response is due to the patient’s health status and disease stage, which are not easily controlled. Another controllable factor is final product potency and consistency, which depends in large part on the functional status of the starting material. These functional properties currently are not well characterized and this needs to be addressed to assure more consistent and effective cell treatments for patients.
Cell therapeutics must adhere to basic principles of pharmacology for clinical benefit. Final product purity, potency, safety and dose/schedule optimization must be addressed to assure clinical benefit. For some cell therapies this is a signficant liability, for example, autologous CAR-T therapy cell doses can vary widely from patient to patient for autologous CAR T therapies. This has major impacts on clinical outcomes in terms of variability in efficacy and safety. Testing strategies to better characterize autologous and allogeneic starting materials for cell therapies will result in more consistent dosing and potency, with improved clinical benefit for patients. Some of these properties include analysis of proliferation potential, effector function, metabolic fitness and immune memory specifically for T cell therapies.
CAR-T immunotherapy challenges
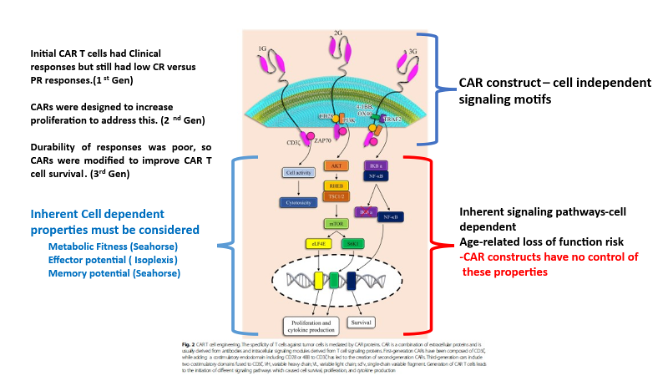
Chimeric Antigen Receptor (CAR) constructs (Fig 1, Marofi et al. Stem Cell Research & Therapy (2021) 12:81) have been undergoing refinements to improve T cell therapies. While improvements in CARs has led to better clinical outcomes, CARs are dependent on the functionality of the inherent signal transduction pathways present in the T cells collected for manufacturing. If these pathways are not functioning optimally, CAR constructs will not give the degree of benefit they are intended to deliver. It is important to better understand the status of the cell starting material for better performance of therapies. This key principle is applicable to all cell therapies, and is not adequately addressed as part of patient/donor screening and manufacturing.
Figure 1. CAR-T therapy mechanistic considerations
API (Active Pharmaceutical Ingredient) considerations
Final product (FP) refers to a well characterized therapeutic preparation containing minimal unrelated contaminant cells to allow a consistent dose of the therapeutic agent. For molecular-based therapies this is termed the Active Pharmaceutical Ingredient (API). The FP should be produced in a consistent manufacturing campaigns for control of potency and dosage administered. API variability in the FP results in variability in therapeutic effect and safety. This can confound clinical outcomes. Control of FP API is a straightforward process for molecular therapies, assuring that the API is uniform in potency and composition. Utilizing the API concept to denote the cellular Active Pharmaceutical Ingredient (cAPI) for the production of consistent therapeutics is needed for cell therapies.
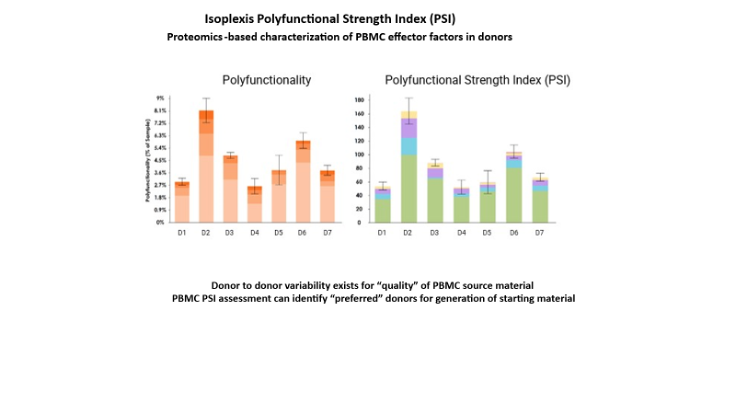
In regards to cAPI, approaches currently use standard starting material collection and processing procedures including donor screening, enrichment of specific cell subsets, expansion protocols and testing of the manufactured products. Better functional characterization of the cAPI to minimize the content of ineffective cells present in the final product is lacking. This impacts the % cAPI present in the final product, which can cause efficacy and safety variability (Nat.Med, doi.org/10.1038/s41591-021-01436-0, Nat Med. 2020, December;26(12):1878–1887. doi:10.1038/s41591-020-1061-7.). Studies have shown that the cAPI content for CAR-T therapies can be a low as 20-25% of the cell dose administered. Carrying out deeper characterization of the patient/donor starting material, manufacturing intermediates and FP can improve this to assure consistent and potent FP. Proteomic studies on effector function cytokine release (PSI) by T cell and TIL products have shown that the percentage of cells retaining the desired effector phenotypes varies. Figure 2 depicts two key characteristics of donor cell variability. The left panel demonstrates the degree of effector function (PSI) variability in the percentage of cells from a healthy donor in terms of the fraction of cells having PSI profiles consistent with T cell activation and effector-related functions, while the right panel depicts the variability of the PSI index for the same donors for their T cell repertoire. This type of analysis facilitates the identification of preferred donors for starting materials to better optimize the production of allogeneic T cell therapeutics and also has autologous applications in patient screening. Implementing this type of analysis at early stages of manufacturing assures the production of cell immunotherapies with potent effector function and better cAPI content.
Figure 2. Donor cell variability
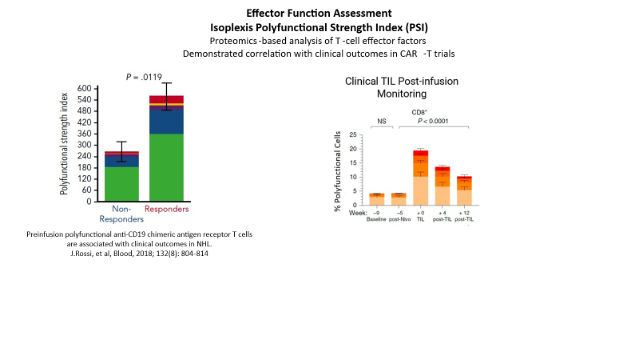
In Figure 3 the left panel demonstrates the correlation between effector function (PSI) and clinical responders or non-responders in patients treated with a CD19 CAR-T cell therapy. The right panel illustrates the variability in the evaluation of TILs post-infusion, indicating that the cAPI content for PSI competent cells comprises less than 20% of the total cell fraction in those patients that receive TIL infusions (https://www.nature.com/articles/s41591-021-01462-y).
Strategies to monitor and improve cAPI content in cellular therapy products
Effector function
A variety of assays have been used to evaluate the effector function of cell therapies. These include cell killing assays, cytokine and cell marker expression analyses. Typically these have not demonstrated a strong correlation with clinical outcomes, but have been used to demonstrate effector potential of the cell therapy. New proteomic assays of effector function have been developed that demonstrate a significant correlation with clinical outcomes in terms of responder and nonresponder endpoints for cell immunotherapies, indicating that effector functions hould be considered for donor screening, testing starting materials, manufacturing intermediates and final product.
Cell metabolism
The metabolic state of cells is a critical component of their effector function, both in Regen Med and immunotherapeutic applications. Specifically, T cell immune responses are dependent on a metabolic shift from oxidative phosphorylation (oxphos) to glycolysis (Rivera et al. Frontiers in Immunology, 1 March 2021 | Volume 12 | Article 645242 ). Quiescent T cells rely on oxphos for energy needs. Upon pathogen-mediated activation, T cells become T effector cells (Teff) and shift to glycolysis for energy production and effector function. Hence, optimal Teff function for the eradication of tumors is dependent on the metabolic shift of Tnaive/mem cells to Teff cells which is mediated by a glycolytic shift in metabolism by these cells. Additionally, glycolysis shifts at the cellular level have been associated with Regen Med cellular responses. These data demonstrate the importance of assessing the metabolic fitness of patient/donor starting materials intended for administration to patients.
Conclusion
Cell therapies are a paradigm shift in medicine, already demonstrating remarkable results in a variety of indications to date with numerous clinical trials ongoing or planned in the near term. Despite these promising results, it is clear that this class of therapeutics can be further optimized to garner even greater clinical benefit. Some key aspects for further improvement include better characterization of the potency and durability of cells from donors, starting materials, manufacturing intermediates and final products manufactured. The technologies to enable this, using metabolic and proteomics-based effector function evaluations, can be leveraged to improve the cAPI composition of the infused product, resulting in greater clinical benefit to the patient.